 OUSD Research and Engineering
OUSD Research and Engineering  West Point
West Point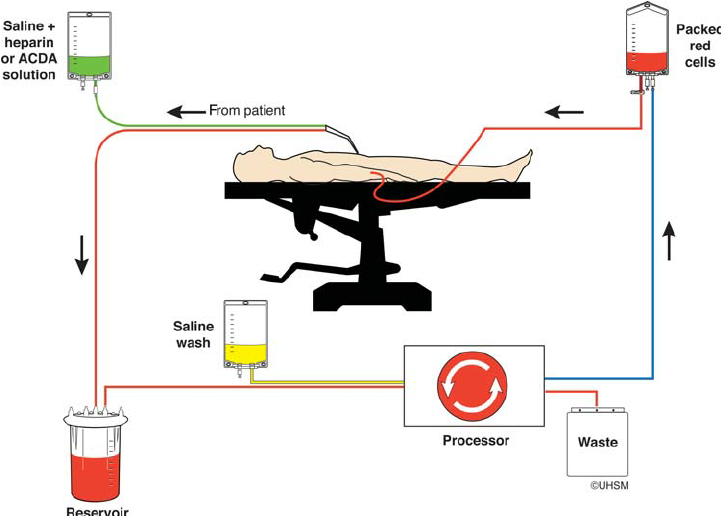
Abstract
Gunshot wounds in the field have potential to result in massive internal or external hemorrhage. The type of bullet tip, projectile, or shrapnel has a large effect on the scale of damage and bleeding, but generally, all uncontrolled large vein or arterial bleeding will lead to fatality. Prevention of hypovolemic shock and death can usually only be achieved by blood transfusion and rapid surgical intervention. One system that has been implemented in the civilian field for help with both massive trauma and use in operative settings is the cell salvage system (CSS). This system utilizes collection techniques to gather lost blood cells, apply anticoagulants to reduce clotting, wash to prevent sepsis, and reinfuse into the patient to help prevent hypoperfusion. Successful integration of a system like this into the field could fill the gap that is left by field medicine when allogeneic blood transfusions are usually not available in preoperative settings, or before reaching the medical treatment facility (MTF). Our project would work on developing techniques to make this system field applicable, with our initial goals to implement into MTFs, followed by medical transports, and finally deployment in the field by ground medical personnel.
Problem Statement
TCCC data show that 90% of combat fatalities succumb to their injuries before reaching a medical treatment center. Of these casualties, the vast majority are caused by external and internal hemorrhage, as well as pneumothorax. What is done by first responders is essential and creating better and more efficient field crafted devices allows for a greater chance for casualties to reach an MTF and eventually decisive surgical facilities.
Proposal
Our proposal is to create a Field Autotransfusion System (FAST).
This system could greatly reduce the amount of combat fatalities related to massive hemorrhage.
FAST would require several components which we can define as several links in our autotransfusion chain: collection, hemo-processing, pumping, and reinfusion.
Collection- We have explored several possible methods of blood collection. First would be direct body to device, where current tools such as decompression needles could be attached to FAST. Second would be a hemo-retentive system to device, where the patient would be placed in a modified stretcher that would collect lost blood and route to FAST. Third would be suction to device method, where lost blood on non-retentive surfaces could be suctioned up and routed to FAST.
Hemo-processing- This part of the chain would involve several important steps to make the blood viable for reinfusion. It would involve the application of low-level anticoagulants to prevent possible blood embolism. Also involved would be blood-washing, using both filter devices and saline wash to prevent sepsis. We have also considered possible re-addition of synthetic clotting factors to prevent coagulopathy.
Pumping- Device power could come from mobile battery packs, hand power cranking, or manual pumping. Ideally flow rate could be maintained through an automatic pressure system.
Reinfusion- Delivery back to the individual via IV or IO access, at a controlled rate from a hemo-processed reservoir.
Challenges and Unknowns
Corporations such as HemoSEP have recently been exploring concepts and technologies related to FAST. Current difficulties they are facing when implementing this system include field testing, possible contamination, and blood-washing efficiency. As opposed to the proposal by HemoSEP in which the system would be implemented first at a field level, our approach would begin with clinical trials at MTFs, then move to medical transportation, and lastly combat field level. We will also be exploring different techniques of collection, blood-washing, and powering to make an ideal system for today's warrior.
Sources:
1. Esper SA, Waters JH. Intra-operative cell salvage: a fresh look at the indications and contraindications. Blood Transfus. 2011;9(2):139-147. doi:10.2450/2011.0081-10 https://ignite.ll.mit.edu/ignite/
2. Hans Hulsebos, MC USN, Jared Bernard, MC USN, Consider Autotransfusion in the Field, Military Medicine, Volume 181, Issue 8, August 2016, Pages e945–e947, https://doi.org/10.7205/MILMED-D-15-00046
3. http://www.naemt.org/Education/IGa%20Intro%20to%20TCCC%20with%20Notes%202-17-09.pdf
4. Gourlay T, Simpson C, Robertson CADevelopment of a portable blood salvage and autotransfusion technology to enhance survivability of personnel requiring major medical interventions in austere or military environmentsBMJ Military Health 2018;164:96-102.
Comments
kcole | 8 February 2021
There are so many examples…
There are so many examples of medical techniques and devices that are driven first by military needs, but benefit all of us. I hope this becomes a standard for emergency medicine some day.
khalilkwok | 14 February 2021
Mr. Cole, Thank you for…
Mr. Cole,
Thank you for your comment and feedback. Much of the inspiration for this system came from experiences in the field of civilian emergency medicine. From your professional bio, we were able to see that you have an incredibly vast array of knowledge and experience, and would appreciate any continued critique and feedback.
dBlocher | 9 February 2021
This is a great well thought…
This is a great well thought out idea! The inclusion of references and research into commercial ventures in the area is impressive. What is your vision with respect to equipment SWaP, and how would required materiel fit into different phases of treatment? Would field medics need to carry pumps and collection bags with them, or what those arrive with a medi-vac? If the blood needed to be processed right away, could the processing device be manufactured in a sufficiently small swap to be man-portable with all the other things soldiers carry? Would blood need to be processed immediately or could that wait until the soldier arrived at a field hospital?
I too hope that a similar break through could be fielded to help save lives.
khalilkwok | 14 February 2021
Dr. Blocher, We appreciate…
Dr. Blocher,
We appreciate your feedback.
DFreinberg | 9 February 2021
Certainly an interesting…
Certainly an interesting concept, Khalil.
I suggest you use a popular military planning tool called the running estimate. List out additional assumptions, facts, and constraints and revisit the list often.
My gut feel is that a hand-crank system or manually operated device is the minimum, perhaps having two ways of pumping the blood through the system is ideal. One of my favorite quotes in regards to engineering redundancy is "One is none, two is one" ... say the electrical system is compromised or the batteries are empty - then you move to manual operation.
I'd challenge you to isolate each issue at a time. What is the best means of blood collection, what is the best way to clean it (and what contaminants may be involved ... dust, oil, etc). You could always build systems that do each function and then figure out how to integrate them later.
khalilkwok | 14 February 2021
Maj. Freinberg, The points…
Maj. Freinberg,
The points you make are incredibly pertinent to the issues we have considered thus far, and we have considered several possible solutions. One of the most important things we would like to address when moving forward is operator preference and current equipment/power capabilities.
1. We are definitely considering having an electrical operating system (depending on the battery size and weight) with a manual operating system as a failsafe (hand pump pressure system).
2. As we move forward we will be addressing issues systematically as you stated, isolating and consulting experts for the problems we may face as we work to make our system field capable.
DFreinberg | 24 February 2021
Looks like I'll be helping…
Looks like I'll be helping you. Note, I've got a background in all sorts of electromechanical devices including liquid level sensors, fluid control devices (aka solenoids), human machine interface proucts, and circuit breakers - all of which may be useful on this application.